Original Article – DOI: 10.33594/000000871
CPB (60): 280 - 290
Accepted: 01.06.2026 - Published: 03.06.2026
Metabolic Syndrome: a Clinical Case Report and Literature Review
bHospital of Vietnam National University (VNU), VNU, Hanoi, Vietnam,
cVietnam National Heart Institute, Bach Mai Hospital, Hanoi, Vietnam,
dDepartment of Internal Medicine, Vietnam University of Traditional Medicine (VUTM), Hanoi, Vietnam,
eBoard of directors, Vietnam University of Traditional Medicine (VUTM), Hanoi, Vietnam
Keywords
Abstract
Background/Aims: To present a clinical case of metabolic syndrome (MetS) and to provide a concise pathophysiological overview with emphasis on underlying metabolic and inflammatory mechanisms. Methods: This study is a case report combined with a focused literature review. We describe a patient with MetS who was evaluated and treated at the Hospital of Vietnam National University in Hanoi, Vietnam. Results: A 20-year-old male presented with headaches and palpitations. Clinical examination revealed obesity (BMI 37.1) with a waist circumference of 111 cm, dyslipidemia (triglycerides/HDL-cholesterol/LDL-cholesterol/total cholesterol: 3.84/1.15/4.39/7.29 mmol/L), and hyperglycemia (blood glucose 7.07 mmol/L, HbA1c 7.2%). The patient also exhibited sinus tachycardia (114 beats/min) and elevated blood pressure (170/102 mmHg left arm, 162/100 mmHg right arm), which was confirmed by 24-hour ambulatory blood pressure monitoring. The triglyceride-to-HDL cholesterol ratio (TG/HDL) was calculated as approximately 3.34, indicating significant insulin resistance and increased cardiovascular risk. Based on these findings, a diagnosis of metabolic syndrome associated with obesity, type 2 diabetes mellitus, and hypertension was established. The clinical phenotype is consistent with adipose tissue dysfunction, chronic low-grade inflammation, and insulin resistance, which contribute to dyslipidemia and activation of neurohormonal pathways such as the renin–angiotensin–aldosterone system. The patient received prompt medical treatment and achieved clinical stabilization. Conclusion: This case highlights the early manifestation of metabolic syndrome and illustrates its underlying pathophysiological mechanisms. Effective management requires early diagnosis and a combined approach including lifestyle modification, weight reduction, and individualized pharmacological therapy to improve metabolic control and reduce the risk of long-term cardiovascular complications.
Introduction
Metabolic syndrome (MetS) is a cluster of interrelated metabolic abnormalities that markedly increase the risk of cardiovascular disease (CVD), type 2 diabetes mellitus (T2D), myocardial infarction, and stroke [1–5]. It is characterized by the coexistence of central obesity, insulin resistance, dyslipidemia, and hypertension, reflecting a complex interaction between metabolic and inflammatory processes. At the mechanistic level, visceral adiposity plays a central role by promoting adipokine imbalance, chronic low-grade inflammation, and impaired insulin signaling, which together contribute to systemic metabolic dysregulation. The concept of MetS has evolved over several decades. Early observations by Kylin and later Vague highlighted the association between hypertension, hyperglycemia, and visceral obesity. Subsequently, Reaven introduced the concept of “Syndrome X,” emphasizing insulin resistance as a key underlying mechanism, while Kaplan described the “Deadly Quartet,” linking obesity, glucose intolerance, dyslipidemia, and hypertension. These developments ultimately led to formal diagnostic criteria established by organizations such as the World Health Organization (WHO) and the International Diabetes Federation (IDF), which have been refined over time to improve clinical applicability [4–6]. Today, MetS represents a major global health challenge, with rapidly increasing prevalence driven by urbanization, sedentary lifestyles, and rising rates of obesity. It is estimated that approximately 25% of the adult population worldwide is affected, with even higher prevalence in older individuals and an increasing incidence among younger populations [6–9]. This trend underscores the importance of early detection and a better understanding of the underlying pathophysiological mechanisms [10-12]. In this context, we present a clinical case of metabolic syndrome in a young patient and discuss the condition from a mechanistic and translational perspective, integrating clinical findings with current knowledge on metabolic and inflammatory pathways.
Clinical Case
A 20-year-old male was admitted to the Hospital of Vietnam National University (Hanoi, Vietnam) in July 2024 with complaints of persistent headaches, fatigue, palpitations, and episodes of rapid heart rate over the preceding eight months. The patient reported intermittent symptoms that initially resolved spontaneously; however, increasing frequency and severity of headaches and palpitations prompted medical evaluation. On physical examination, blood pressure was markedly elevated at 170/102 mmHg in the left arm and 162/100 mmHg in the right arm after rest, with a heart rate of 118 beats/min. The patient appeared fatigued and exhibited severe obesity with a body mass index (BMI) of 37.1 (height 165 cm, weight 101 kg) and a waist circumference of 111 cm. Laboratory investigations revealed normal hematological parameters, while biochemical analysis demonstrated hyperglycemia with elevated HbA1c, hyperuricemia, and significant dyslipidemia characterized by increased triglycerides, total cholesterol, and LDL cholesterol (Table 1). Echocardiography demonstrated preserved left ventricular ejection fraction (EF 65.6%) (Fig. 1), while abdominal ultrasound findings were consistent with fatty liver (Fig. 2). Electrocardiography showed sinus tachycardia (Fig. 3). Doppler ultrasound of the renal arteries was unremarkable. In addition, 24-hour ambulatory blood pressure monitoring confirmed persistent hypertension with elevated systolic and diastolic values (Fig. 4).
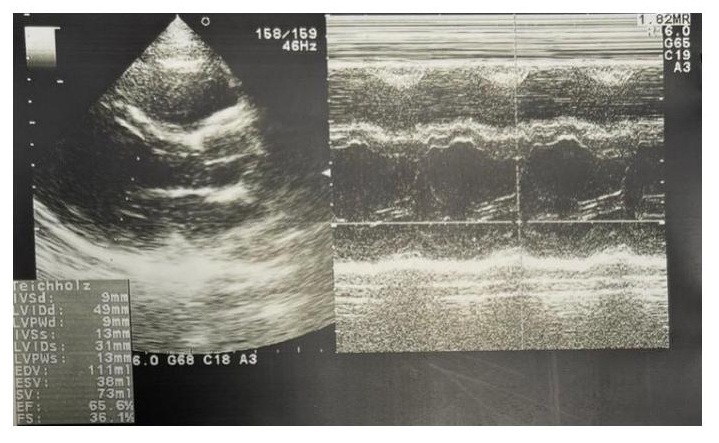
Fig. 1: Result of Echocardiogram.
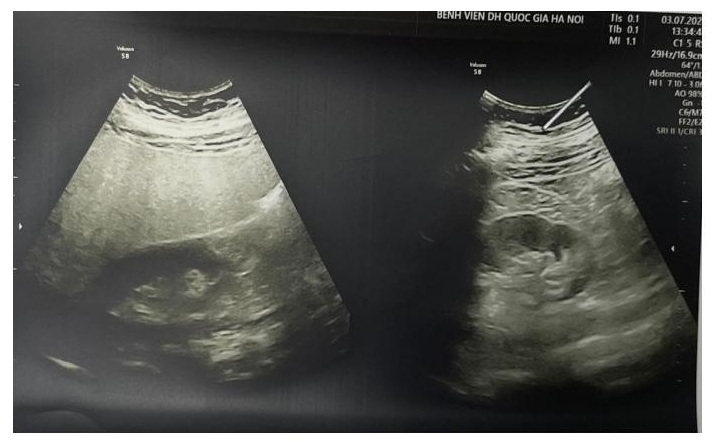
Fig. 2: Result of Abdominal Ultrasound.
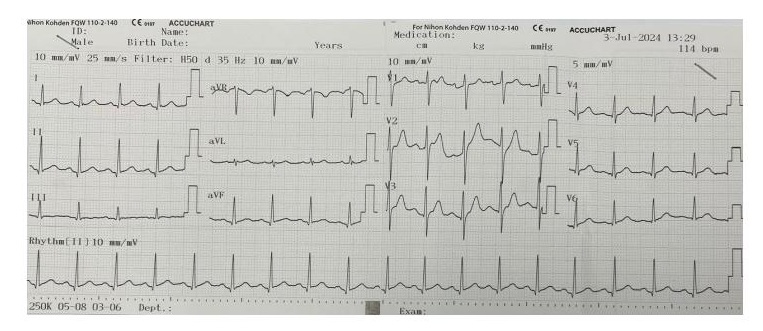
Fig. 3: Electrocardiogram.
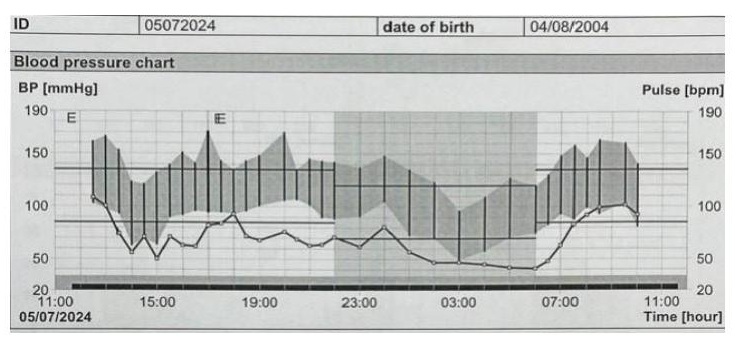
Fig. 4: 24-Hour Blood Pressure Monitoring.
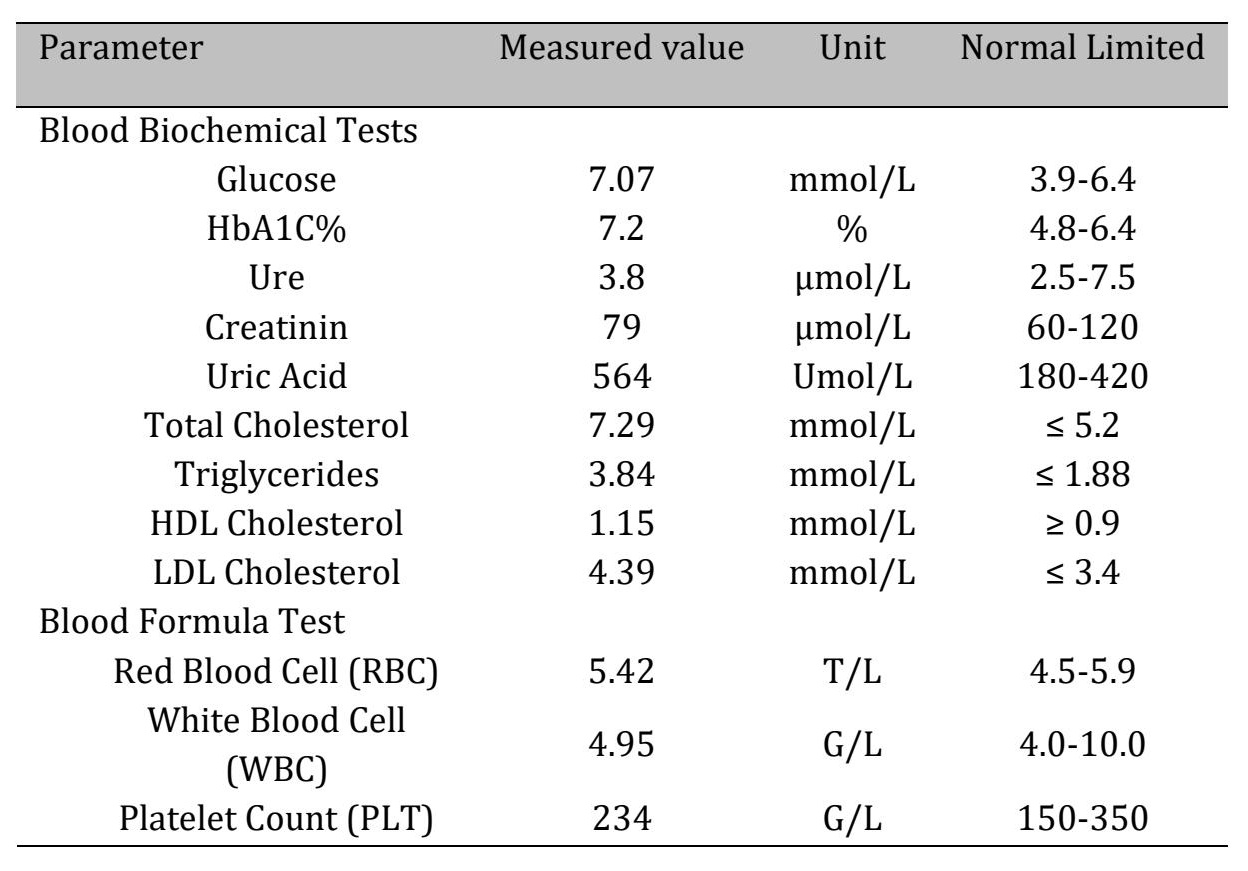
Table 1: Result of Blood Tests
Metabolic syndrome (MetS) is a cluster of interrelated metabolic abnormalities that significantly increase the risk of cardiovascular disease (CVD), type 2 diabetes mellitus (T2D), and stroke. It is defined by the coexistence of central obesity, hypertension, hyperglycemia, and dyslipidemia, typically characterized by elevated triglycerides and reduced HDL cholesterol levels. The development of MetS is closely associated with overweight, obesity, and a sedentary lifestyle, with visceral adiposity playing a central role. The distribution and amount of adipose tissue, particularly increased waist circumference, are key determinants of metabolic risk. Excess abdominal fat leads to increased release of free fatty acids into the portal circulation, promoting lipid accumulation in the liver and skeletal muscle and contributing to metabolic dysfunction. At the mechanistic level, MetS arises from a complex interaction between genetic predisposition and environmental factors. Chronic low-grade inflammation is a central feature, characterized by increased levels of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), which impair insulin signaling pathways. This results in insulin resistance, reduced glucose uptake, and compensatory hyperinsulinemia. In parallel, adipose tissue dysfunction leads to adipokine imbalance, further exacerbating metabolic disturbances [12]. These processes contribute to dyslipidemia, endothelial dysfunction, and the development of hypertension. In addition, metabolic alterations are associated with elevated uric acid levels, increased fibrinogen and plasminogen activator inhibitor-1 (PAI-1), reflecting a prothrombotic and inflammatory state. Hormonal and stress-related factors may further aggravate insulin resistance and metabolic imbalance [3–5, 13].
Risk Factors for Metabolic SyndromeThe development of metabolic syndrome is influenced by a combination of demographic, genetic, and lifestyle-related factors. Age is a major determinant, with prevalence increasing significantly in older populations, although MetS is increasingly observed in younger individuals due to rising obesity rates. Sex-related differences have also been reported, with a particularly high prevalence in postmenopausal women, likely reflecting hormonal changes that influence fat distribution and insulin sensitivity. Genetic predisposition plays an important role, as individuals with similar environmental exposures may exhibit different susceptibility and age of onset, indicating a complex interaction between genetic background and lifestyle factors. Environmental influences such as urbanization, dietary habits, reduced physical activity, and increased caloric intake further contribute to the rising global prevalence of MetS. Overweight and obesity, particularly visceral adiposity, represent central risk factors. Adipose tissue functions as an active endocrine organ, releasing free fatty acids and adipokines that promote systemic inflammation, insulin resistance, and atherogenic processes. In addition, several comorbid conditions are closely associated with MetS. Obstructive sleep apnea contributes to intermittent hypoxia and sympathetic activation, thereby increasing cardiovascular risk. Non-alcoholic fatty liver disease reflects underlying metabolic dysfunction and is strongly linked to insulin resistance and chronic inflammation. Chronic kidney disease is associated with vascular calcification and metabolic disturbances that further exacerbate cardiovascular risk. Endocrine factors also play a role, including polycystic ovary syndrome in women and reduced testosterone levels in men, both of which are associated with insulin resistance and adverse metabolic profiles.
Diagnosis of Metabolic SyndromeEarly identification of metabolic syndrome is essential in clinical practice. Initial assessment typically includes evaluation of medical and family history, measurement of blood pressure, and assessment of central obesity using waist circumference. In individuals with risk factors such as obesity, family history of type 2 diabetes, or sedentary lifestyle, further laboratory evaluation of fasting glucose and lipid profile is recommended. The diagnosis of MetS is based on established clinical criteria, most commonly those proposed by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III). According to these criteria, the presence of at least three of the following components is required: central obesity, elevated blood pressure, hyperglycemia, hypertriglyceridemia, and reduced HDL cholesterol levels (Table 2). Epidemiological studies have demonstrated that the prevalence of MetS increases with age and is strongly associated with obesity and body mass index. In addition, there is growing evidence that metabolic syndrome may develop early in life, particularly in overweight and obese adolescents, highlighting the importance of early screening and prevention strategies [14, 15]. Recent updates in diagnostic criteria have focused on refining thresholds and improving applicability across different populations. For example, the impaired fasting glucose threshold has been lowered to 100 mg/dL (5.6 mmol/L) in accordance with updated ADA and WHO recommendations. Furthermore, adaptations of diagnostic criteria for specific populations, including children and different ethnic groups, have been proposed to better reflect variations in body composition and metabolic risk.
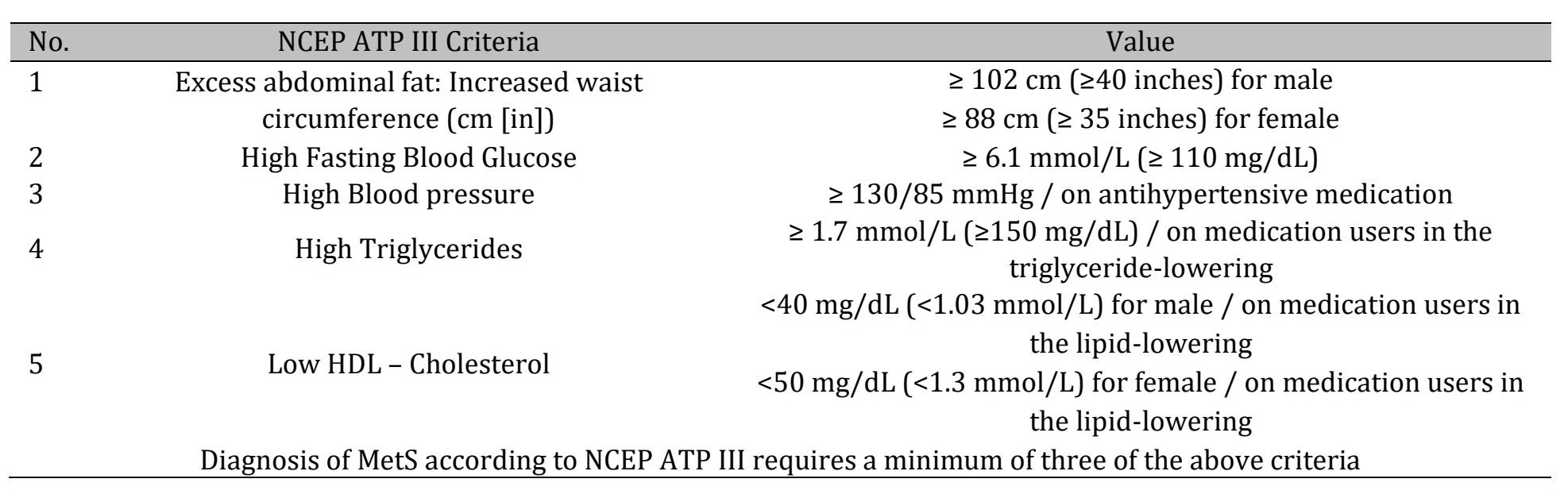
Table 2: Commonly Used Criteria for Diagnosing Metabolic Syndrome
The management of metabolic syndrome requires a comprehensive approach combining lifestyle modification and, when necessary, pharmacological therapy. The primary goal is to improve metabolic parameters, reduce cardiovascular risk, and target the underlying mechanisms such as insulin resistance and chronic low-grade inflammation. Lifestyle modification represents the cornerstone of treatment. A heart-healthy diet with reduced intake of saturated fats and simple sugars, combined with increased consumption of fruits, vegetables, legumes, and whole grains, is strongly recommended. Regular physical activity, including aerobic and resistance exercise, should be performed for at least 30 minutes on most days of the week. Even in the absence of significant weight loss, increased physical activity can improve insulin sensitivity and cardiovascular outcomes [7–9]. For overweight and obese individuals, a weight reduction of 7–10% over 6–12 months has been shown to significantly improve metabolic parameters and may partially reverse components of MetS [9, 13, 16]. Additional measures include smoking cessation and stress management, both of which contribute to improved cardiovascular and metabolic health. Personalized treatment strategies should be developed based on individual risk factors and comorbidities [4, 16, 17]. Pharmacological therapy is indicated when lifestyle interventions alone are insufficient. Anti-obesity medications, including glucagon-like peptide-1 (GLP-1) receptor agonists such as liraglutide and semaglutide, as well as other agents, may support weight reduction. Hypertension is typically managed with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) as first-line therapy, often in combination with calcium channel blockers or other antihypertensive agents. Dyslipidemia is primarily treated with statins, with additional agents such as fibrates considered in selected cases. For impaired glucose metabolism or type 2 diabetes, medications such as metformin or other insulin-sensitizing agents are commonly used to improve glycemic control [9, 16, 17].
Discussion
The present case illustrates an early manifestation of metabolic syndrome in a young patient, characterized by the coexistence of central obesity, hypertension, hyperglycemia, and dyslipidemia. Clinical findings, including elevated blood pressure, sinus tachycardia, and metabolic abnormalities (Fig. 1–4, Table 1), indicate a state of systemic metabolic dysregulation. According to the NCEP ATP III criteria, the presence of at least three components is sufficient for diagnosis; in this case, the patient fulfilled four criteria, including central obesity, hypertension, hypertriglyceridemia, and type 2 diabetes mellitus (Table 2). Further analysis of lipid parameters revealed a triglyceride-to-HDL cholesterol ratio (TG/HDL) of approximately 3.34, which is markedly elevated and widely recognized as a surrogate marker of insulin resistance and increased cardiovascular risk. This finding supports the presence of significant underlying metabolic impairment and an atherogenic lipid profile. From a mechanistic perspective, the clinical phenotype observed in this patient can be explained by adipose tissue dysfunction associated with visceral obesity. Increased release of free fatty acids into the portal circulation promotes lipid accumulation in the liver and skeletal muscle (Fig. 2), while adipokine imbalance and chronic low-grade inflammation impair insulin signaling pathways. This results in insulin resistance, reduced glucose uptake, and compensatory hyperinsulinemia. These processes contribute to dyslipidemia, endothelial dysfunction, and activation of neurohormonal pathways such as the renin–angiotensin–aldosterone system, ultimately leading to hypertension and systemic metabolic imbalance. To further support this interpretation, publicly available gene expression data from adipose tissue in obesity and insulin resistance (GEO dataset GSE20950) demonstrate upregulation of pro-inflammatory cytokines such as IL6 and TNF, as well as alterations in adipokine-related genes including LEP and ADIPOQ [18]. These molecular findings are consistent with the mechanisms described above and align with the clinical presentation of the patient (Fig. 5). As illustrated in diagram of pathophysiological Mechanism [12], these interconnected mechanisms provide a conceptual framework linking visceral obesity to insulin resistance, dyslipidemia, and hypertension. In parallel, pathophysiological Mechanism summarizes the broader pathophysiological pathways underlying metabolic syndrome, highlighting the interaction between metabolic, inflammatory, and neurohormonal processes [12]. The early onset of metabolic syndrome in this patient underscores the growing impact of obesity and sedentary lifestyle on younger populations. In addition to metabolic disturbances, elevated uric acid levels and prothrombotic factors such as fibrinogen and plasminogen activator inhibitor-1 further reflect the systemic nature of the disorder. Treatment of metabolic syndrome requires a combination of lifestyle modification and pharmacological intervention [25-29]. In this case, the patient was successfully managed with antihypertensive and heart rate–controlling therapy, including calcium channel blockade, angiotensin receptor blockade, and beta-blockade, resulting in clinical stabilization [40-48]. Long-term management included a combination of antihypertensive therapy (amlodipine/valsartan), lipid-lowering therapy (statin), and antidiabetic treatment (empagliflozin/metformin), along with lifestyle interventions focusing on weight reduction, diet, and physical activity [4], [16], [17], [49-62]. Weight reduction plays a central role in improving metabolic outcomes. Previous studies have demonstrated that even moderate weight loss is associated with significant reductions in blood pressure and improvement in metabolic parameters. Mechanistically, reduction of visceral fat decreases activation of the renin–angiotensin–aldosterone system and improves insulin sensitivity [44], [62]. Pharmacological considerations are particularly important in patients with obesity and metabolic syndrome [44], [62]. While beta-blockers effectively reduce heart rate, alternative agents such as ivabradine may be considered in selected cases to avoid potential metabolic side effects. Similarly, antihypertensive and antidiabetic therapies should be selected with consideration of their metabolic profiles and impact on insulin sensitivity [1], [9]. Overall, this case highlights the importance of early diagnosis and comprehensive management of metabolic syndrome, integrating clinical findings with mechanistic understanding to improve long-term outcomes (Fig. 5).
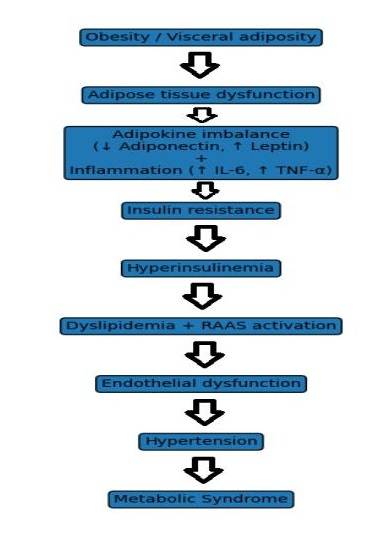
Fig. 5: Metabolic Syndrome Schematic Fig. to Summarize the proposed pathophysiological mechanisms.
Conclusion
This case highlights the early manifestation of metabolic syndrome in a young patient and underscores the importance of timely diagnosis and intervention. The markedly elevated triglyceride-to-HDL cholesterol ratio supports the presence of significant insulin resistance and an atherogenic metabolic profile. Effective management of metabolic syndrome requires an integrated approach combining lifestyle modification and individualized pharmacological therapy. Weight reduction plays a central role in improving metabolic and cardiovascular parameters, while appropriate treatment of hypertension and hyperglycemia is essential to prevent disease progression. Overall, this case emphasizes the need for early detection and a mechanistic understanding of metabolic syndrome to guide targeted interventions and reduce the risk of long-term cardiovascular complications.
Disclosure Statement
The authors have no competing interests.
References
- Alberti KG, Zimmet PZ. Diagnosis and classification of diabetes mellitus and its complication. Part 1: Diagnosis and classification of diabetes mellitus provisional of WHO consultation. Diabet Med 1998; 15: 539-53. https://doi.org/10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
- Expert panel of detection, evaluation and treatment of high blood cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert. Panel on detection, evaluation and treatment of high bloob cholesterol in Adults (Adults treatment panel III). JAMA 2001; 285 (19): 2486-2497. https://doi.org/10.1001/jama.285.19.2486
- Sulistiowati Eva, Sihombing M. NCEP-ATP III and IDF criteria for metabolic syndrome predict type 2 diabetes mellitus. Universa Medicina 2016; 35 (1): 46-55. https://doi.org/10.18051/UnivMed.2016.v35.46-55
- Grundy SM, Cleerman JI, Dniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association Heart. Lung, and Blood Insitute Science Statement, Circulation 2006; 112, pp. 2735. https://doi.org/10.1161/CIRCULATIONAHA.105.169404
- Earl S Ford, Wayne H Giles, William H Dietz. Prevalence of the metabolic syndrome among US adults: Finding from the third National Health and Nutrition Examination Survey. JAMA 2002; 287 (3): 356-359. https://doi.org/10.1001/jama.287.3.356
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363 (9403): 157-163. https://doi.org/10.1016/S0140-6736(03)15268-3
- Mann T, Tomiyama AJ, Westling E, et al. Medicare's search for effective obesity treatments: Diets are not the answer. Am Psychol 2007; 62 (3): 220-233. https://doi.org/10.1037/0003-066X.62.3.220
- Ross R, Neeland IJ, Yamashita S, et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS [International Atherosclerosis Society] and ICCR [International Chair on Cardiometabolic Risk] Working Group on Visceral Obesity. Nat Rev Endocrino 2020; l16 (3): 177-189. https://doi.org/10.1038/s41574-019-0310-7
- Omair A Shariq, Travis J Mckenzie. Obseity-related hypertension: a review of pathophysiology, management, and the role of metabolic surgery. Gland Surg. 2020; 9 (1): 80-93. https://doi.org/10.21037/gs.2019.12.03
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and the American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract 2016; 22 (Suppl 3): 1-203. https://doi.org/10.4158/EP161365.GL
- Luo J, Hendryx M, Laddu D, et al. Racial and ethnic differences in anthropometric measures as risk factors for diabetes. Diabetes Care 2019; 42 (1): 126-133. https://doi.org/10.2337/dc18-1413
- Harrison's principles of Internal medicine 18th Edition (2012). The metabolic syndrome.
- US Preventive Services Task Force. Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults. JAMA 2018; 320 (11): 1163-1171. https://doi.org/10.1001/jama.2018.13022
- Cook S, Weitzman M, Auinger P, et al. Prevalence of a Metabolic Syndrome Phenotype in Adolescents: Findings From the Third National Health and Nutrition Examination Survey, 1988-1994. Arch Pediatr Adolesc Med. 2003; 157 (8): 821-827. https://doi.org/10.1001/archpedi.157.8.821
- Alkhatib B, Orabi A, Agraib Lana M, Al-Shami Islam. Journal of the Egyptian Public Health Association 2024, 99: 34. https://doi.org/10.1186/s42506-024-00181-9
- Jordan J, Astrup A, Engeli S, et al. Cardiovascular effects of phentermine and topiramate: A new drug combination for the treatment of obesity. J Hypertens 2014; 32 (6): 1178-1188. https://doi.org/10.1097/HJH.0000000000000145
- Arnett DK, Blumenthal RS, Albert, MA, et al. ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019; 140 (11): e596-e646. https://doi.org/10.1161/CIR.0000000000000725
- Aditya Saxena, Kumar Sachin. A Network Biology Approach for Assessing the Role of Pathologic Adipose Tissues in Insulin Resistance Using Meta-analysis of Microarray Datasets. Curr Genomics. 2018; 19 (7): 630-666. https://doi.org/10.2174/1389202919666180726125645
- Carey RM, Calhoun DA, Bakris GL, Brook RD, Daugherty SL, Dennison-Himmelfarb CR, Egan BM, Flack JM, Gidding SS, Judd E, Lackland DT, Laffer CL, Newton-Cheh C, Smith SM, Taler SJ, Textor SC, Turan TN, White WB., American Heart Association Professional/Public Education and Publications Committee of the Council on Hypertension; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Genomic and Precision Medicine; Council on Peripheral Vascular Disease; Council on Quality of Care and Outcomes Research; and Stroke Council. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association. Hypertension. 2018 Nov;72(5):e53-e90. https://doi.org/10.1161/HYP.0000000000000084
- Puttnam R, Davis BR, Pressel SL, Whelton PK, Cushman WC, Louis GT, Margolis KL, Oparil S, Williamson J, Ghosh A, Einhorn PT, Barzilay JI., Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) Collaborative Research Group. Association of 3 Different Antihypertensive Medications With Hip and Pelvic Fracture Risk in Older Adults: Secondary Analysis of a Randomized Clinical Trial. JAMA Intern Med. 2017 Jan 01;177(1):67-76.https://doi.org/10.1001/jamainternmed.2016.6821
- Wright JT, Probstfield JL, Cushman WC, Pressel SL, Cutler JA, Davis BR, Einhorn PT, Rahman M, Whelton PK, Ford CE, Haywood LJ, Margolis KL, Oparil S, Black HR, Alderman MH., ALLHAT Collaborative Research Group. ALLHAT findings revisited in the context of subsequent analyses, other trials, and meta-analyses. Arch Intern Med. 2009 May 11;169(9):832-42.https://doi.org/10.1001/archinternmed.2009.60
- Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O'Brien E, Ostergren J., ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 2005 Sep 10-16;366(9489):895-906.https://doi.org/10.1016/S0140-6736(05)67185-1
- Weber MA, Jamerson K, Bakris GL, Weir MR, Zappe D, Zhang Y, Dahlof B, Velazquez EJ, Pitt B. Effects of body size and hypertension treatments on cardiovascular event rates: subanalysis of the ACCOMPLISH randomised controlled trial. Lancet. 2013 Feb 16;381(9866):537-45.
- https://doi.org/10.1016/S0140-6736(12)61343-9
- ONTARGET Investigators. Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, Schumacher H, Dagenais G, Sleight P, Anderson C. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008 Apr 10;358(15):1547-59.
- Khan N, McAlister FA. Re-examining the efficacy of beta-blockers for the treatment of hypertension: a meta-analysis. CMAJ. 2006 Jun 06;174(12):1737-42.https://doi.org/10.1503/cmaj.060110
- Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure-lowering treatment on cardiovascular outcomes and mortality: 14 - effects of different classes of antihypertensive drugs in older and younger patients: overview and meta-analysis. J Hypertens. 2018 Aug;36(8):1637-1647. https://doi.org/10.1097/HJH.0000000000001777
- Lindholm LH, Carlberg B, Samuelsson O. Should beta blockers remain first choice in the treatment of primary hypertension? A meta-analysis. 2005 Oct 29-Nov 4 Lancet. 366(9496):1545-53. https://doi.org/10.1016/S0140-6736(05)67573-3
- Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11, 000 participants from 42 trials. Am J Med. 2009 Mar;122(3):290-300. https://doi.org/10.1016/j.amjmed.2008.09.038
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T, Mahfoud F, Redon J, Ruilope L, Zanchetti A, Kerins M, Kjeldsen SE, Kreutz R, Laurent S, Lip GYH, McManus R, Narkiewicz K, Ruschitzka F, Schmieder RE, Shlyakhto E, Tsioufis C, Aboyans V, Desormais I., ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018 Sep 01;39(33):3021-3104. https://doi.org/10.1201/9780429199189-75
- James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC, Svetkey LP, Taler SJ, Townsend RR, Wright JT, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014 Feb 05;311(5):507-20. https://doi.org/10.1001/jama.2013.284427
- Jamerson K, Weber MA, Bakris GL, Dahlöf B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ., ACCOMPLISH Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008 Dec 04;359(23):2417-28. https://doi.org/10.1056/NEJMoa0806182
- Bakris GL, Sarafidis PA, Weir MR, Dahlöf B, Pitt B, Jamerson K, Velazquez EJ, Staikos-Byrne L, Kelly RY, Shi V, Chiang YT, Weber MA., ACCOMPLISH Trial investigators. Renal outcomes with different fixed-dose combination therapies in patients with hypertension at high risk for cardiovascular events (ACCOMPLISH): a prespecified secondary analysis of a randomised controlled trial. Lancet. 2010 Apr 03;375(9721):1173-81. https://doi.org/10.1016/S0140-6736(09)62100-0
- Phillips CO, Kashani A, Ko DK, Francis G, Krumholz HM. Adverse effects of combination angiotensin II receptor blockers plus angiotensin-converting enzyme inhibitors for left ventricular dysfunction: a quantitative review of data from randomized clinical trials. Arch Intern Med. 2007 Oct 08;167(18):1930-6. https://doi.org/10.1001/archinte.167.18.1930
- Huxel C, Raja A, Ollivierre-Lawrence MD. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): May 22, 2023. Loop Diuretics.
- Sica DA, Carter B, Cushman W, Hamm L. Thiazide and loop diuretics. J Clin Hypertens (Greenwich). 2011 Sep;13(9):639-43. https://doi.org/10.1111/j.1751-7176.2011.00512.x
- Chapman N, Dobson J, Wilson S, Dahlöf B, Sever PS, Wedel H, Poulter NR., Anglo-Scandinavian Cardiac Outcomes Trial Investigators. Effect of spironolactone on blood pressure in subjects with resistant hypertension. Hypertension. 2007 Apr;49(4):839-45. https://doi.org/10.1161/01.HYP.0000259805.18468.8c
- Khosla N, Kalaitzidis R, Bakris GL. Predictors of hyperkalemia risk following hypertension control with aldosterone blockade. Am J Nephrol. 2009;30(5):418-24. https://doi.org/10.1159/000237742
- Williams B, MacDonald TM, Morant S, Webb DJ, Sever P, McInnes G, Ford I, Cruickshank JK, Caulfield MJ, Salsbury J, Mackenzie I, Padmanabhan S, Brown MJ., British Hypertension Society's PATHWAY Studies Group. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015 Nov 21;386(10008):2059-2068. https://doi.org/10.1016/S0140-6736(15)00257-3
- Akbari P, Khorasani-Zadeh A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jan 23, 2023. Thiazide Diuretics.
- McKeever RG, Hamilton RJ. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 5, 2022. Calcium Channel Blockers.
- Herman LL, Padala SA, Ahmed I, Bashir K. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 31, 2023. Angiotensin-Converting Enzyme Inhibitors (ACEI).
- Farzam K, Jan A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 22, 2023 Beta Blockers.
- Herman LL, Bruss ZS, Tivakaran VS. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Mar 28, 2023. Hydralazine.
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda (MD): Jan 8, 2018. Alpha 1 Adrenergic Receptor Antagonists.
- Bulsara KG, Cassagnol M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jan 22, 2023. Amlodipine
- Khan KM, Patel JB, Schaefer TJ. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): May 23, 2023. Nifedipine.
- Talreja O, Cassagnol M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 28, 2023. Diltiazem
- Fahie S, Cassagnol M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 6, 2023 Verapamil.
- Hill RD, Vaidya PN. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Mar 27, 2023 Angiotensin II Receptor Blockers (ARB)
- Yasaei R, Saadabadi A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 17, 2023. Clonidine.
- Taylor BN, Cassagnol M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 10, 2023. Alpha-Adrenergic Receptors.
- Leung AA, Wright A, Pazo V, Karson A, Bates DW. Risk of thiazide-induced hyponatremia in patients with hypertension. Am J Med. 2011 Nov;124(11):1064-72. https://doi.org/10.1016/j.amjmed.2011.06.031
- Desai AS, Swedberg K, McMurray JJ, Granger CB, Yusuf S, Young JB, Dunlap ME, Solomon SD, Hainer JW, Olofsson B, Michelson EL, Pfeffer MA., CHARM Program Investigators. Incidence and predictors of hyperkalemia in patients with heart failure: an analysis of the CHARM Program. J Am Coll Cardiol. 2007 Nov 13;50(20):1959-66. https://doi.org/10.1016/j.jacc.2007.07.067
- Patel P, Nessel TA, Kumar D D. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 4, 2023. Minoxidil.
- Goyal A, Cusick AS, Thielemier B. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jun 26, 2023. ACE Inhibitors.
- Almajid AN, Cassagnol M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Oct 10, 2022. Amiloride.
- Kandler MR, Mah GT, Tejani AM, Stabler SN, Salzwedel DM. Hydralazine for essential hypertension. Cochrane Database Syst Rev. 2011 Nov 09;(11):CD004934. https://doi.org/10.1002/14651858.CD004934.pub4
- Iyer P, Dirweesh A, Zijoo R. Hydralazine Induced Lupus Syndrome Presenting with Recurrent Pericardial Effusion and a Negative Antinuclear Antibody. Case Rep Rheumatol. 2017; 2017: 5245904. https://doi.org/10.1155/2017/5245904
- Manzon L, Nappe TM, DelMaestro C, Maguire NJ. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jun 26, 2023. Clonidine Toxicity.
- Yang CH, Raja A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Mar 13, 2023. Terazosin.
- Xi L, Qingxing X, Xiaohui P, et al. Type 2 diabetes mellitus in adults: pathogenesis, prevention and therapy. Signal Transduction and Targeted Therapy. 2024; 9: 262. https://doi.org/10.1038/s41392-024-01951-9